TECHNICAL STUDY
Multiple scenarios are common during the loading and unloading of cots in the back of emergency service vehicles. This, coupled with patient weight, can make the job of the medic very difficult and results in poor ergonomics and higher lumbar and joint stresses1 . At some angles, the cot may not load into the fastener or loading system at all. The purpose of this study was twofold: 1) to evaluate the angles at which an emergency cot would no longer load into the fastener or loading system, and 2) to determine the forces (pounds-force: lbf or Newtons: N) required to load and unload the cot at these angles.
Methods
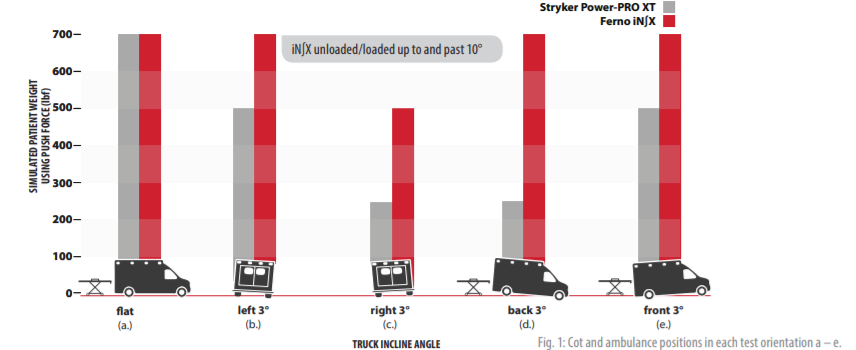
Two emergency cots were loaded and unloaded into a simulated ambulance in this study. The FERNO iN∫X Intergrated Patient Transport & Loading System (Wilmington, OH) and the Stryker Power-PRO XT (Portage, MI) cot were kept on a horizontal position, and a simulated ambulance was placed at a nominal height per the ambulance floor height standard2. Six ambulance floor orientations were tested (Figure 1,2). When viewed from the rear as if loading/unloading a cot, the ambulance floor was adjusted either a) parallel to the horizontal, b) at –3 degree increments when viewed from left to right, or c) at +3 degree increments from left to right. When viewed from the side, the floor was also adjusted either d) at –3 degree increments when viewed from rear to front, or e) at +3 degree increments. When both the cot and the floor were placed on the horizontal, multiple cot approach angles were also tested (Figure 2). iN∫Line (FERNO) and Power-LOAD (Stryker) fasteners were mounted to the simulated ambulance floor per manufacturer’s installation instructions. Simulated patient weights of 0, 250, 500, and 700 lbf (0, 1112, 2224, and 3114 N) were placed on the cot patient surface in all scenarios, respectively. The full weight capacity of each cot was 700 pound-force (lbf or 3114 N). The maximum force required to unload or load the cot into the fastener was measured using a load cell (accuracy ±0.1% of readout) placed coaxial to medic pull or push directions.
Results
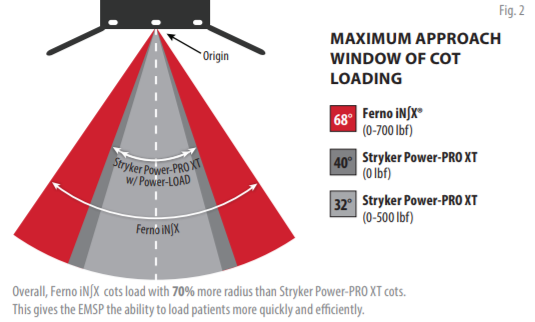
Both cots unloaded and loaded comparably when parallel with the ground and were able to do up to the maximum load of 700 lbf (3,114 N) at the (a) orientation. There was no functional difference between these forces for the iN∫X (unloading: 24.7 lbf [110 N]; loading: 17.6 lbf [78 N]) and Power-PRO XT (unloading: 22.2 lbf [99 N]; loading: 12.8 lbf [57 N]) at this unloaded baseline condition. In the (b) orientation of –3 degrees, the Power-PRO XT could not be unloaded or loaded when 700 lbf (3114 N) was placed on the patient surface. The iN∫X unloaded and loaded up to and past –10 degrees under 700 lbf (3114 N) of load, and required 125.4 lbf (558 N) (unloading) or 114.9 lbf (511 N) (loading) to do so. In the (c) orientation of +3 degrees, the Power-PRO XT could not be unloaded or loaded at the 500 lbf (2224 N) or 700 lbf (3114 N) loads. The iN∫X unloaded and loaded up to 500 lbf (3114 N) and required 106.4 lbf (473 N) (unloading) or 57.6 lbf (256 N) (loading) to do so. It should be noted that the (c) orientation resulted in the right side of the simulated ambulance floor to be above the nominal height standard (see Figure 1c above). In the (d) orientation of –3 degrees, the Power-PRO XT could not be unloaded or loaded at the 500 lbf (2224 N) or 700 lbf (3114 N) loads. At 700 lbf (3114 N) of load the iN∫X unloaded and loaded with 152.5 lbf (678 N) (unloading) or 111.7 lbf (497 N) (loading). At 700 lbf (3114 N) of load there was a statistically significant difference between the forces required to unload the Power-PRO XT versus iN∫X cot in the (e) orientation (p < 0.05); the Power-PRO XT cot required 79% more force to unload (111.2 lbf [495 N] versus 62.0 lbf [276 N]). The Power-PRO XT would not load in this orientation at 700 lbf (3114 N); the iN∫X loaded under 107.3 lbf (477 N) of force. Looking at Figure 2, the maximum approach angle capability of the Power-PRO XT cot and Power-LOAD fastener was found to be load dependent (p < 0.05), and ranged from a radius of 32 degrees at full capacity to a radius of 40 degrees with an unloaded cot. The iN∫X and iN∫Line system was capable of a 68 degree radius, off-axis approach angle, regardless of the load on the patient surface.
Conclusion
If an emergency cot and ambulance floor are at different angles with respect to one another, such as is often the case when parked on a hill, driveway, or curb, or if the medic approaches the back of the ambulance at a slightly off axis angle, then the unloading and loading dynamics of the cot are changed. In some cases, the cot will not load at all, even with medic assistance. There was a twofold increase in the off-axis loading capability with the iN∫X versus the Power-PRO XT cot, and assistance was needed for angles higher than 3 degrees or with heavy patient weights when the Power-PRO XT cot was used. At offset approach angles, cot choice can leave the medic with up to a 79% increase in load to bear. A cot with greater forgiveness with regard to off-axis mismatch of the cot/fastener interface proved beneficial to the medic. In addition, the -3 degree orientation gives the iN∫X ability to load up to 10 degrees, giving the medic greater flexibility in loading at greater angles.
KEY DEFINITIONS
“N”=“Newton”—the standard unit of force in the International System of Units.LBF—The pound-force (symbol: lbf, or lbf) is a unit of force.
For purposes of this white paper, LBF represents “simulated patient weights,” and “N,” or “Newtons”, is used as a unit of measurement during loading and unloading of both evaluated systems.
[1] Fredericks et. al. 2013 [2] Federal Specification for the Star-of-Life Ambulance, KKK-A-1822.